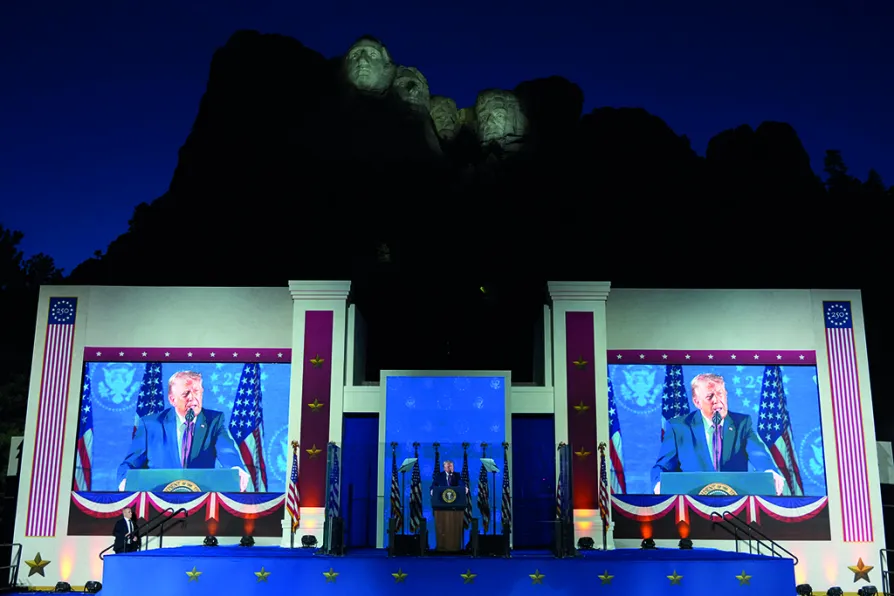
CJ ATKINS takes a closer look at Trump’s recent spate of red-baiting speeches and asks why the authoritarian president is running scared

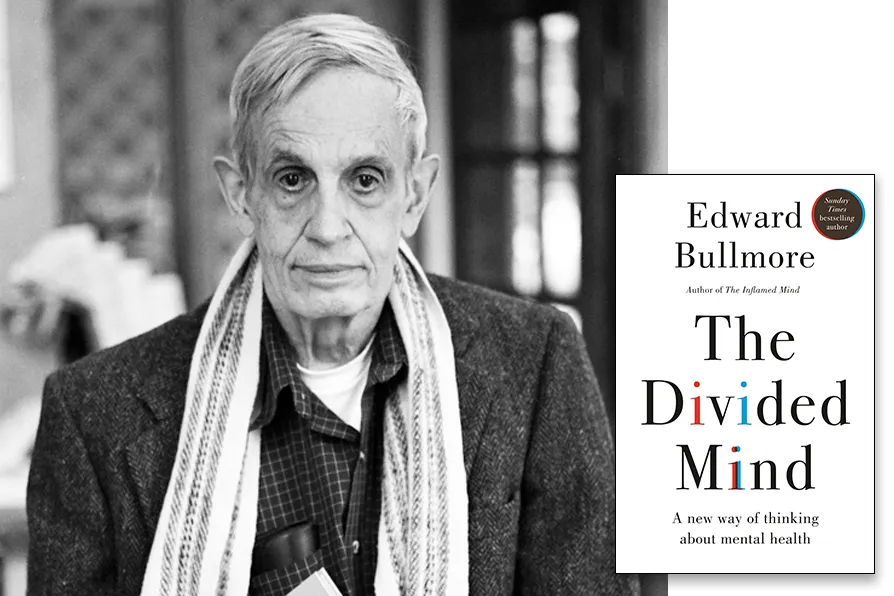
The traumatic power struggle within mental health
ALASTAIR KEMP and RUTH HUNT explain how ideological differences about the causes of mental illness have been leveraged to make the case for cutbacks

JOHN McINALLY sees little chance of change at Westminster, and calls on the left to get serious about building a real alternative
With the centenary of the UN Slavery Convention upon us, ROGER McKENZIE argues much needs to be done to rid us of all its contemporary manifestations
SEVIM DAGDELEN says European Nato states are escalating ever closer to direct conflict with a nuclear power, and sacrificing welfare states built up over a century to finance it
CLAUDIA WEBBE says the horrific price British patients will pay for this NHS deal is now clear — and there’s time to get out of it, if MPs will only force the issue
KENNY MacASKILL says the lines between party, government and Civil Service in Scotland have been blurred and we need a thorough investigation into how






ONE of the most vitriolic power struggles between professional groups is happening now and goes to the very essence of what is, or is not, mental illness.
Squaring off against each other are those who believe in a biomedical or genetic basis to mental illness (in the main, psychiatrists) and those who believe mental illness is a natural response to a threat or trauma (mainly psychologists).
At the root of it, is the battle between professions for legitimacy. Who should be controlling the narrative and who should be informing policy? Yet forgotten are the service users who are most affected by such policy arguments at this level.

Similar stories
RICHARD SHILLCOCK examines an enjoyable, but philosophically conventional book, and urges Marxists to employ their capacity to embrace the totality in any explanation
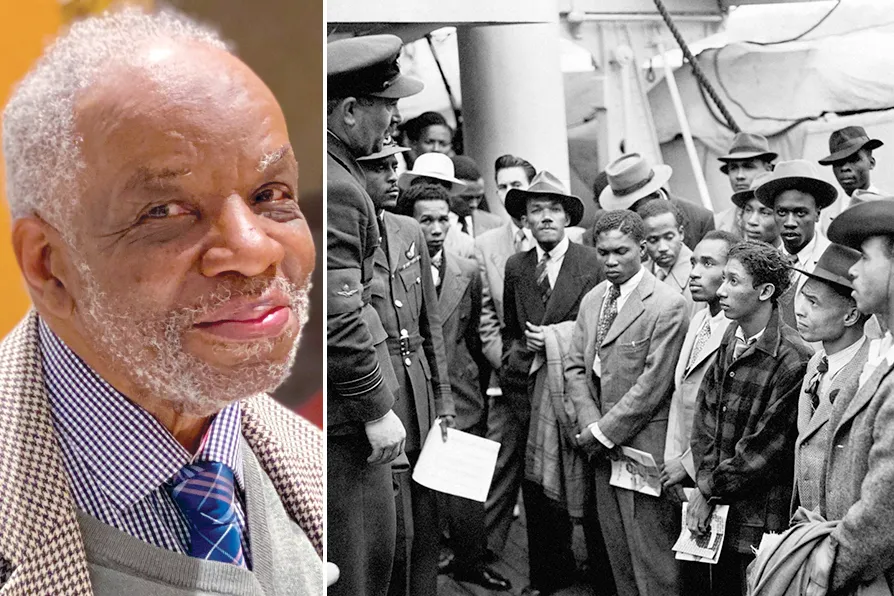
1943-2025: How one man’s unfinished work reveals the lethal lie of ‘colour-blind’ medicine
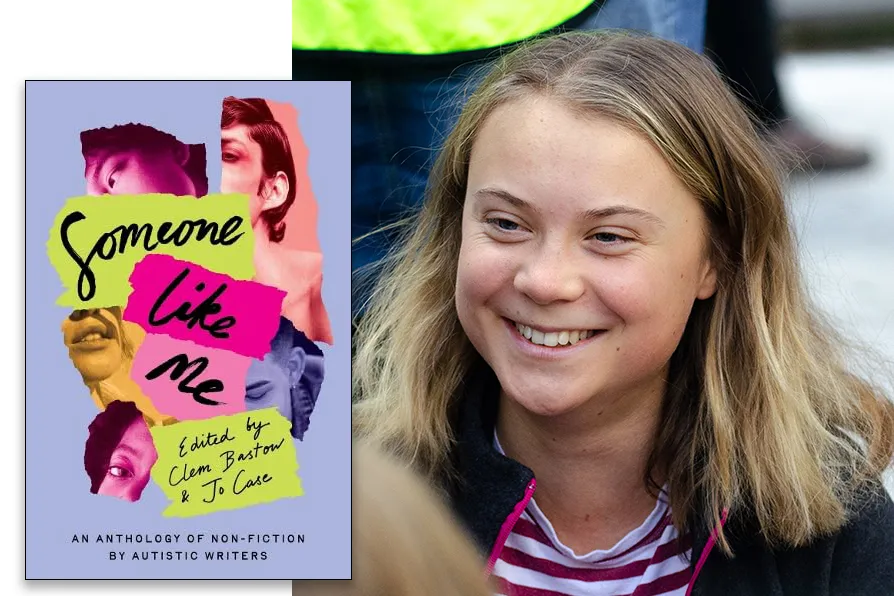
JOSEPHINE BARBARO welcomes a diverse anthology of experiences by autistic women that amounts to a resounding chorus, demanding to be heard

A new report from the Citizens Advice destroys the government narrative about disabled people ‘choosing’ not to work, showing the £3,000 annual cuts will create a two-tiered system based on claim dates rather than needs, writes DYLAN MURPHY