PCS general secretary FRAN HEATHCOTE explains why opposing war is inseparable from defending jobs, wages and public services – and why readers should come to the London Peace Conference on Saturday June 20

The scourge of restrictive practices in mental health care: ‘It just muted me’
The lack of NHS mental health provision for young people has led to many placements, out of sight and out of mind, in so-called ‘specialist,’ privately run units. This comes at great cost for all involved, writes RUTH HUNT


As protests erupt over Henry Nowak’s murder, ANDREW MURRAY argues that anger is being exploited to advance a wider racist and anti-immigration agenda
CARLOS MARTINEZ explains the sound case for car manufacturing co-operation with China
The National Emergency Briefing outlines the need for urgent action to address environmental crisis, says PAUL DONOVAN, warning that there’s no time to indulge the arguments of the fossil-fuel-funded climate-change deniers
Campaigners say criticism of Labour MP Stephen Morgan’s position on Gaza has been met with police intervention and cancelled opportunities for debate. HESTER WOLFE reports
The Committee for the Defence of Iranian People’s Rights warns of escalation danger in Iran war






ALTHOUGH the NHS hands over vast sums to independent mental health service providers, those who have lost loved ones or have been damaged by long periods of restrictive practices, often have to fight to be even acknowledged — let alone get real justice.
For those who have been in these units either as patients or staff, there’s a feeling of relief they have survived. But they also have a need to share their stories, to add further weight to the call to shut these expensive units down and end unsafe restrictive practices.
Steph had a dream of working in mental health, using her own personal experiences and in turn, helping those who are going through similar turmoil.

Similar stories

Gisele Pelicot said ‘shame must change sides.’ We may think we agree, but, argues LOUISE RAW, society still has some way to go
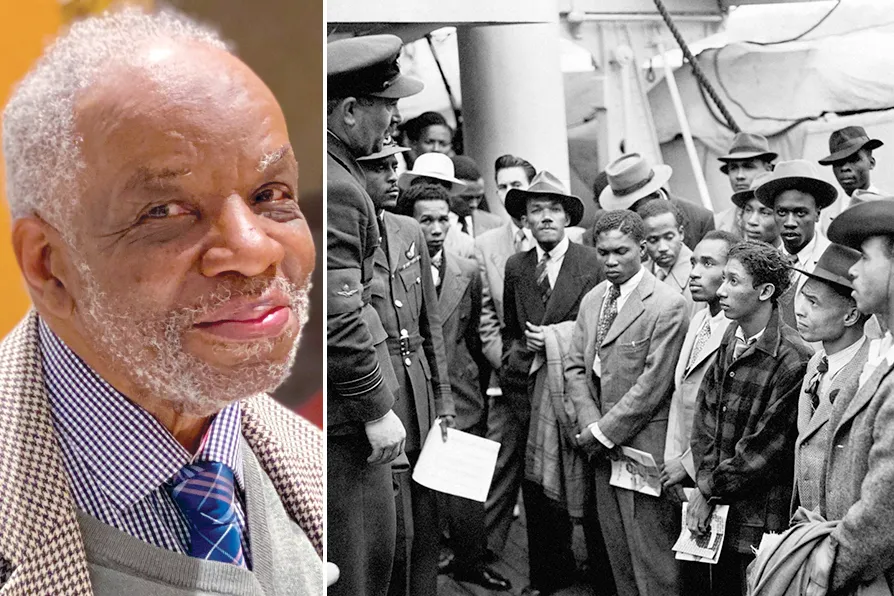
1943-2025: How one man’s unfinished work reveals the lethal lie of ‘colour-blind’ medicine
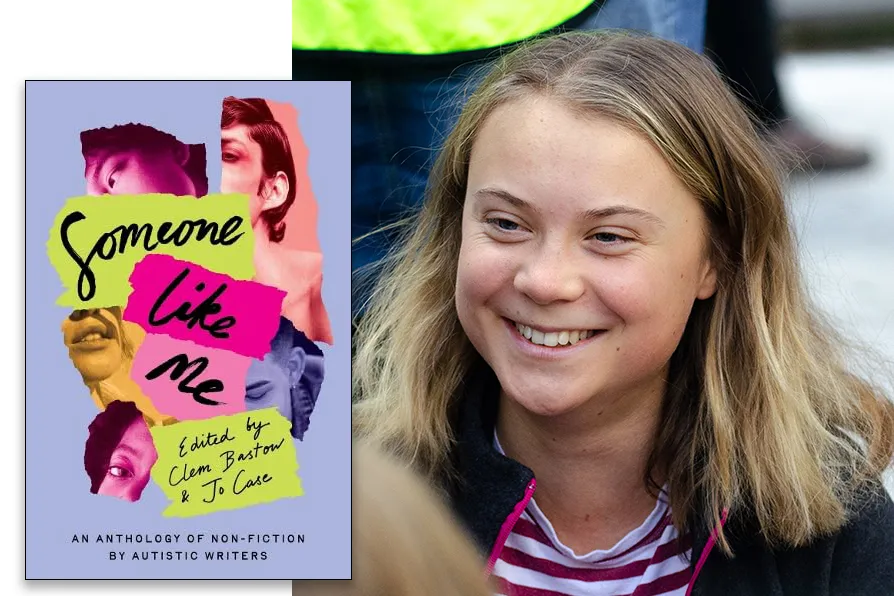
JOSEPHINE BARBARO welcomes a diverse anthology of experiences by autistic women that amounts to a resounding chorus, demanding to be heard

Seventeen years after losing her council job due to needing endometriosis surgery, Michelle Dewar’s campaign for paid menstrual leave gained 50,000 signatures in a week, reports ELIZABETH SHORT